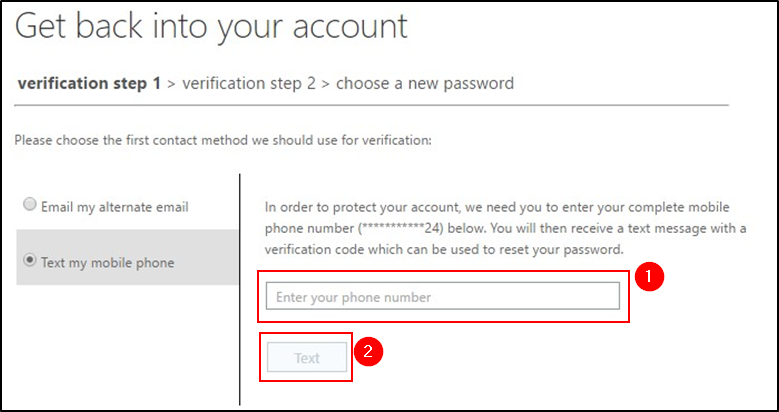
2. Verification codes will be sent to the mail address and cell phone number that you provided in the onboarding process.
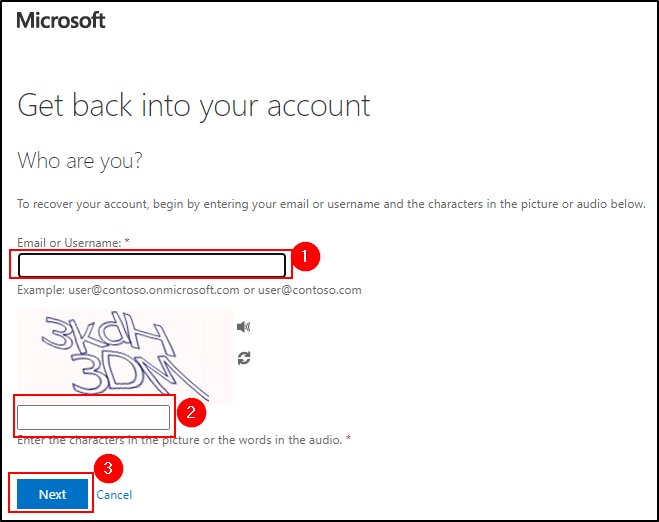
Enter your full mail address/cell phone number and the codes in the password reset dialog windows accordingly.
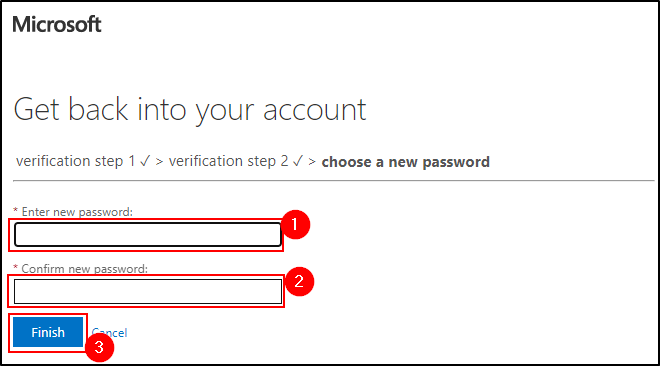
3. After you successfully passed the verification steps, you can set a new password.
4. The password will be set. After 15 minutes it will be fully replicated, and you can login using your new password.
Frequent questions and answers:
Every employee must change his/her Windows/domain-password after 180 days at the latest. As a result, all further passwords (for SAP, Intranet and www/Internet) are synchronized automatically (but please consider the password-rules (see next point)). Changing your password before the end of 180 days is certainly possible.
The new password management requires a minimum length of 10 characters, that the password has to be changed after 180 days and mustn’t correspond with the last 5 passwords. The password must meet 3 out of 4 of the following requirements:
The information and documents contained on the following pages of this website are for information purposes only. These materials do neither constitute an offer nor an invitation to subscribe to or to purchase securities, nor any investment advice or service, and are not meant to serve as a basis for any kind of obligation, contractual or otherwise. Securities may not be offered or sold in the United States of America (“US”) absent registration under the US Securities Act of 1933, as amended, or an exemption from registration. The securities described on the following pages are not offered for sale in the US or to "US persons" (as defined in Regulation S under the US Securities Act of 1933, as amended).
THE FOLLOWING INFORMATION AND DOCUMENTS ARE NOT DIRECTED AT AND ARE NOT INTENDED FOR USE BY (I) PERSONS WHO ARE RESIDENTS OF OR LOCATED IN THE US, CANADA, JAPAN OR AUSTRALIA OR WHO ARE US PERSONS (AS DEFINED IN REGULATION S UNDER THE US SECURITIES ACT OF 1933, AS AMENDED), OR (II) PERSONS IN ANY OTHER JURISDICTION WHERE THE COMMUNICATION OR RECEIPT OF SUCH INFORMATION IS RESTRICTED IN SUCH A WAY THAT PROVIDES THAT SUCH PERSONS SHALL NOT RECEIVE IT. SUCH PERSONS, OR PERSONS ACTING FOR THE BENEFIT OF ANY SUCH PERSONS, ARE NOT PERMITTED TO VISIT THE FOLLOWING PAGES OF THE WEBSITE.
To visit the following parts of this website you must confirm that
(i) you are not a resident of the United States of America, Canada, Japan or Australia or a "US person" (as defined in Regulation S under the US Securities Act of 1933, as amended),
(ii) you are not a person to whom the communication of the information contained on the website is restricted,
(iii) you will not distribute any of the information and documents contained thereon to any such person, and
(iv) you are not acting for the benefit of any such person.
By clicking on the "Accept" button below, you will be deemed to have made this confirmation.
NOT FOR RELEASE, PUBLICATION OR DISTRIBUTION, DIRECTLY OR INDIRECTLY, IN OR INTO THE UNITED STATES OF AMERICA, AUSTRALIA, CANADA OR JAPAN.
Fresenius has offered its shareholders a scrip dividend for the first time this year. This gave shareholders the opportunity to exchange part of their dividend entitlement for Fresenius shares during the subscription period from May 16 to May 30, 2022, and thus reinvest directly into the Company. Investors have chosen this option for a total of 40 % of shares carrying dividend rights. This means that around 147 million euros will remain within the company.
Based on the acceptance rate, around 4.7 million new shares will be issued, increasing the total number of Fresenius shares to 563,237,277.
The new shares are expected to be credited to the securities accounts of participating shareholders on June 13, 2022. Shareholders who have not or only partially exercised their option will receive the cash dividend also on or around June 13, 2022. The total cash distribution this year amounts to around 367 million euros.
The Else Kröner-Fresenius-Foundation has fully participated in the scrip dividend.
This announcement does not contain or constitute an offer of, or the solicitation of an offer to buy or subscribe for, securities to any person in Australia, Canada, Japan, or the United States of America (the “United States”) or in any jurisdiction to whom or in which such offer or solicitation is unlawful. The securities referred to herein may not be offered or sold in the United States or to, or for the account or benefit of, U.S. persons, absent registration under the U.S. Securities Act of 1933, as amended (the “Securities Act”) except pursuant to an exemption from, or in a transaction not subject to, the registration requirements of the Securities Act. The securities referred to herein may not be offered or sold in Australia, Canada or Japan or to, or for the account or benefit of, any national, resident or citizen of Australia, Canada or Japan. The offer and sale of the securities referred to herein has not been and will not be registered under the Securities Act or under the applicable securities laws of Australia, Canada or Japan. There will be no public offer of the securities in the United States.
June 13, 2022
|
Rancho Palos Verdes, USA
Goldman Sachs 43rd Annual Global Healthcare Conference
PEMEtrexed for injection, a drug used to treat adult patients with lung cancer and malignant pleural mesothelioma, is now available from Fresenius Kabi in the United States. This is the newest addition to the company’s portfolio of generic IV oncology products - the largest such portfolio in the U.S.